
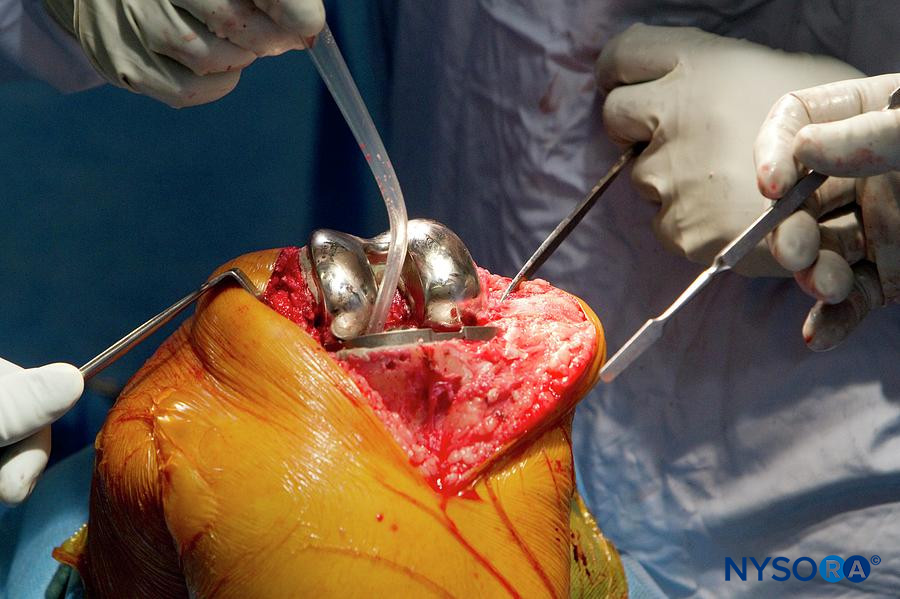
Analgesia for knee surgery, skin anesthesia of the medial aspect of the leg below the knee.
Indications: Analgesia for knee surgery, skin of the medial aspect of the leg below the knee (e.g., ankle or foot surgery). Can be combined with sciatic nerve block for surgery below the knee (e.g., foot amputation, ankle fracture).
Goal: Depending on the level of block, local anesthetic spread around the femoral nerve in the femoral triangle or saphenous nerve in the adductor canal.
Transducer: Linear or curved (larger patients)
Needle: 22 G, 5-8 cm.
Local anesthetic volume: 10 mL
Functional anatomy
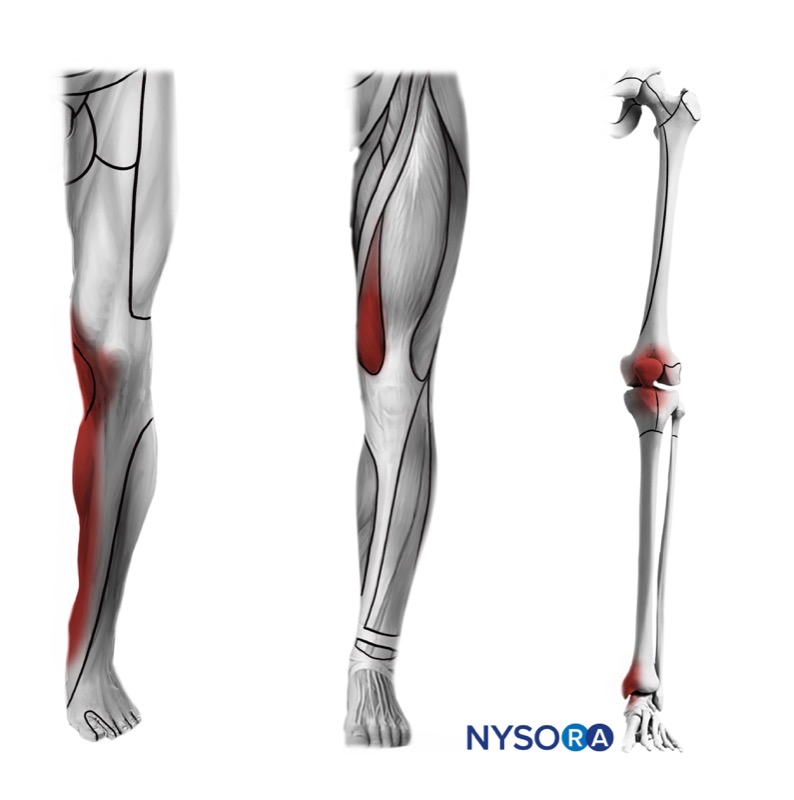
The saphenous nerve is a terminal sensory branch of the femoral nerve. It innervates the medial aspect of the leg distally to the level of the medial ankle and/or midfoot. It supplies sensory branches to the superficial structures of the knee (skin and patellar branches). Saphenous nerve can be blocked at proximal or distal levels (above or below the knee), depending on the indication.


In the proximal thigh, the saphenous nerve travels together with the femoral vessels in the femoral triangle and into the adductor canal under the sartorius muscle.
Femoral triangle limits:
Important FACT: The apex of the femoral triangle defines the proximal end of the adductor canal.
Bottom line: A femoral TRIANGLE injection can block more femoral branches to the knee. An adductor canal injection blocks primarily the saphenous nerve.
Definitions clarification: The femoral triangle ends distally as the adductor canal. Adductor canal is sometimes confusingly referred to as “subsartorius canal”, although the sartorius muscle is the roof in both – femoral triangle and adductor canal.
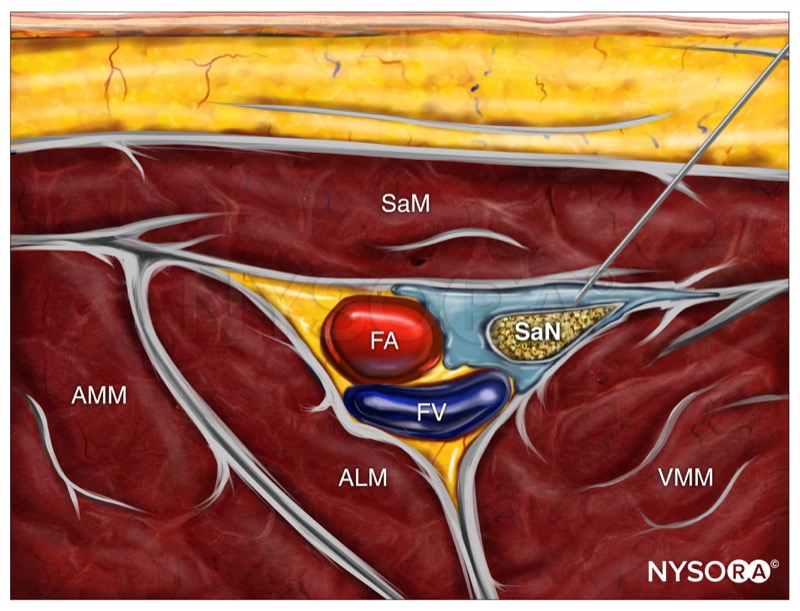
What is in the canal? The bottom line is that adductor canal contains saphenous nerve and femoral artery in a triangular fascial plane made by the sartorius (superficially), the vastus medialis (anterolaterally) and the adductor longus and adductor magnus (posteromedially).
Triangle versus Canal: The femoral triangle is more proximal and contains proximal saphenous nerve, often a branch to the vastus medialis, and sometimes a branch of the obturator nerve, all of which can be involved in contributing innervation to the knee joint. The adductor canal contains distal saphenous nerve, often with medial femoral cutaneous nerve, and may convey injections into popliteal fossa.


Saphenous nerve block at the adductor canal results in anesthesia of the skin from the medial aspect of the leg and knee to the ankle joint and foot.
You should also know: Injection of larger volumes of local anesthetic (e.g., >15 mL) in the adductor canal or femoral triangle may result in a partial block of the quadriceps muscle due to spread around the femoral nerve. Larger volumes of injectate into the adductor canal may also result in spread into the popliteal fossa and popliteal plexus – a group of autonomic and genicular nerves that contribute sensory branches to the posterior capsule of the knee.
Patient position: Supine, with the thigh abducted and externally rotated to allow access to the medial thigh. If unable, separation of the legs may be adequate.
External landmarks: Middle third of the thigh.



Transducer position
Place the transducer in a transverse orientation at the level of the middle third of the thigh (medial side).

Scanning
Identify the correct place for injection by following these steps:
1. Identify the femoral artery deep to the sartorius muscle.


2. Identify the limits of the femoral triangle and adductor canal by scanning up and down until the medial border of the sartorius muscle meets the medial border of the adductor longus muscle.
3. From this point, continue to scan distally until the adductor longus muscle (ALM) becomes shorter in the ultrasound image, and the artery is located in the middle of the sartorius muscle (see the example below). This location is an adequate site for injection – adductor canal.


Needle insertion






